
When people hear the phrase “Tommy John surgery,” they tend to assume it’s one single procedure with one predictable outcome. In reality, that phrase has become a kind of shorthand for several very different surgeries involving the ulnar collateral ligament of the elbow. Over the last decade in particular, the options have expanded, the techniques have evolved, and the recovery timelines have changed dramatically. That’s why you’ll hear one athlete talk about being back on the mound in six months while another is staring down a year and a half of rehab, even though both are said to have “had Tommy John.”
The original Tommy John surgery, the one that dates back to the 1970s, is what surgeons now call a UCL reconstruction. In this procedure, the damaged ligament isn’t fixed or patched up. It’s replaced entirely. The surgeon removes the compromised UCL and reconstructs a new one using a tendon graft harvested from either somewhere else in the athlete’s body or from a cadaver (someone else’s graft). Most commonly the graft is pulled from your forearm or the hamstring. The tendon is then threaded through bone tunnels drilled into the ulna and humerus, essentially creating a brand-new ligament. The body then has to biologically accept and remodel that graft over time. This is a long process, which is why the recovery timeline for a full reconstruction is typically measured in a year or more, especially for pitchers.

For a long time, this was the only real option. If you tore your UCL, especially as a pitcher, reconstruction was the gold standard. It worked, it was durable, and it saved careers. The downside, of course, was how invasive it was and how long the rehab took. You weren’t just healing a ligament. You were waiting for an entirely new piece of tissue to integrate into bone and adapt to the stresses of throwing a baseball at high velocity. Even today, reconstruction still has the longest track record and is often the best option for athletes with chronic damage, poor tissue quality, or years of wear and tear on the elbow.
Over time, surgeons began to notice something important. Not all UCL injuries look the same. Some tears are acute and clean, especially in younger athletes. Instead of the ligament slowly fraying over years, it might pull off the bone in a single moment. In those cases, the ligament tissue itself can still be healthy. That observation opened the door to a different approach: repair instead of reconstruction.
UCL repair is exactly what it sounds like. Rather than replacing the ligament, the surgeon preserves it and reattaches the torn portion back to the bone. Early versions of UCL repair, however, didn’t have great results. Without reinforcement, the repaired ligament was vulnerable during the healing process, and failure rates were higher. That’s where the internal brace comes in, and this is where a lot of modern confusion around “Tommy John surgery” begins.
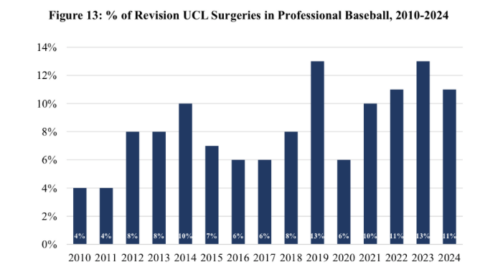
It might be worth noting that in todays game we see re-tearing happen a lot at the higher level. athletes are having a second Tommy John Surgery in their pro career. With the increased rate of Tommy John Surgery happening across the game and the re-tearing at the professional level, it’s obvious why a new form of Tommy John has been pushed.
The internal brace is a strong, collagen-coated suture tape that is anchored across the repaired ligament. It acts like a seatbelt. It’s not meant to permanently replace the ligament or take full loads forever. Instead, it protects the healing tissue during the most vulnerable early phase of rehab. The athlete’s own ligament still does the long-term work, but the brace allows that ligament to heal in a safer, more controlled environment. Because the native anatomy is preserved and no graft has to biologically incorporate, the recovery timeline can be dramatically shorter.
This is why you sometimes hear about pitchers returning to competitive throwing in six to nine months after “Tommy John surgery.” In almost every one of those cases, what they actually had was a UCL repair with an internal brace. It’s still elbow surgery. It’s still serious. But it’s not the same operation that requires a full year and a half of rehab. The key, though, is that not everyone is a candidate. Repair with an internal brace works best in younger athletes with acute tears and good ligament quality. It’s much less effective in elbows that have been breaking down over time.
There are also situations where a surgeon may combine techniques. In some reconstructions, an internal brace is added alongside the tendon graft. The idea is to provide extra stability early on and potentially allow for a more confident rehab progression. However, this doesn’t magically turn a reconstruction into a six-month recovery. The graft still needs time to heal and mature, and the overall timeline remains much closer to that of a traditional Tommy John. The internal brace in this context is more of a supplement than a shortcut.
What complicates all of this is language. Fans, media members, and even athletes often use “Tommy John” as a blanket term. It doesn’t distinguish between reconstruction and repair. It doesn’t tell you whether an internal brace was used. It doesn’t explain whether the ligament was replaced or preserved. As a result, comparisons can be misleading. One pitcher’s comeback story might sound miraculous, while another’s absence feels endless, even though both are described in the exact same way.

The decision about which surgery to perform is ultimately based on what the surgeon sees in the elbow. The location of the tear matters. The quality of the ligament tissue matters. The age of the athlete, their throwing history, and whether the injury is acute or chronic all matter. A clean tear near the bone in a young pitcher with a healthy ligament may be an excellent candidate for repair with an internal brace. A veteran pitcher with years of accumulated stress and a frayed ligament is far more likely to need a full reconstruction.
It’s also worth noting that while reconstruction has decades of data behind it, repair with internal bracing is still relatively new in the big picture. The early and mid-term results have been very encouraging, but long-term durability is still being studied. That doesn’t make it risky or experimental, but it does mean that surgeons are careful about who they recommend it for. Done on the right patient, it can be a career-saver with a much faster return. Done on the wrong patient, it can fail.
So when someone says an athlete “had Tommy John,” the real question should be, “Which one?” Was the ligament replaced, or was it repaired? Was an internal brace used, or not? Those details tell you far more about what the athlete went through and what their road back is going to look like than the name of the surgery ever could. Tommy John surgery isn’t one thing anymore, and understanding that difference helps make sense of why recoveries can look so wildly different from one athlete to the next.

Want to get started training KP? We offer training options in (Tampa FL) for both healthy athletes seeking performance and injured athletes looking for PT.
For more on our Physical Therapy Click Here
To learn more about our performance training Click Here






